12 Jan The Curious Case of CBN & Sleep
Dr. Matt Elmes is a cannabinoid scientist and cannabis enthusiast. His PhD and postdoctoral work focused on the biochemistry of cannabinoids and he made impactful research contributions prior to transitioning to a non-academic career in the California cannabis industry.
You hear it from your buddies and your budtenders alike. If you’re looking to cannabis to better your sleep, then CBN (cannabinol) is the cannabinoid for you!
As both a cannabis scientist and a product formulator within the cannabis industry, I’ve spent a considerable amount of time looking into the validity of these soporific claims. I find the minor cannabinoids to be fascinating and I always like to review what objective evidence we have substantiating a given effect that they may produce. Despite the overwhelming reputation CBN has for improving sleep, I was surprised to find little real data in the published literature to actually support those claims.
My sentiments were echoed in a recent review article, published in the journal Cannabis and Cannabinoid Research, which lays out a scientific summary of nearly all the high-quality human research that has been published around CBN.[1] Allow me to reiterate the author’s points and include some additional thoughts of my own with the hope that this will help readers form an educated opinion about CBN.
First things first: What is CBN?

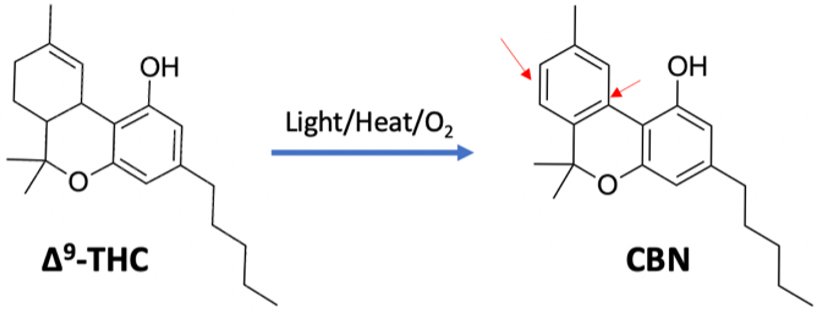
Cannabinol was the very first cannabinoid to be isolated from the cannabis plant in the late 1800s. We have since learned that CBN is a degradant product of THC. This means that THC will slowly transform into CBN over time as cannabis ages. Older bud will generally contain higher CBN levels at the expense of its THC content. Light and heat will accelerate this conversion process, which is part of the reason it’s typically recommended to store your cannabis in a cool, dark place.
Laboratory studies show that CBN interacts with our CB1 cannabinoid receptors about 10 times weaker than ∆9–THC. Due to this CB1 affinity, CBN probably does have some weak psychoactive properties in humans (more on why I say “probably” later in this article). CBN binds to CB2 receptors with greater affinity compared to CB1, so there is reason to believe that it could have some beneficial anti-inflammatory effects similar to THC.
Scientists are able to determine how tightly a compound attaches to a receptor. This is expressed as a Ki (pronounced “Kay-Eye”) value. A lower number indicates stronger binding, which usually means higher potency for a drug. ∆9–THC’s binding affinity to the CB1 receptor = 21nM (nanomolar); this is roughly 10 times stronger than CBN’s binding affinity to CB1, which = 211nM.[2,3] CBN’s binding affinity for CB2 receptors is comparatively a bit stronger, with CB2 Ki = 126nM.[2]
What Does the Research Say About CBN & ZZZ’s?
I don’t want to put too much emphasis on all the preclinical CBN research that’s been done in animals because what occurs in a rodent all too frequently translates poorly to what happens in a human. The most important and relevant points from the animal data is that they generally agree that CBN shows weak cannabimimetic activity (i.e., exhibits weak THC-like effects in tests that have been developed to gauge CB1 receptor activation). However, there does not seem to be a strong consensus one way or the other on CBN’s effects on sleep. Some studies have found that CBN increased barbiturate-induced sleep time (in a rodent model), but other studies seem to contradict those findings[3,4]. CBN did not appear to have any effect at all when given to monkeys.[5]
In a similar vein, I’ll only be discussing in-human CBN research that is of high-quality. Not all research that’s performed is of the same caliber. Various observational or survey-based studies have concluded efficacy of CBN for sleep (such as here and here). However, these studies are frequently funded by industry players with vested interests and often do not have a sufficient quality of study design to put much stock in their results or conclusions. If the research is not peer-reviewed, relies solely on self-reported subjective measurements, and does not include any placebo control, then the ‘results’ don’t carry much weight.
Here’s why: If you give almost any patient population a CBN tincture and ask them to “take it daily and report how much it improved their sleep,” the results will almost always come back positive, even if the effects are neutral in reality. If you instead gave those patients a cannabinoid-free tincture (aka a placebo) but lie and tell the participants that it contains CBN, those results will almost always be positive too! Simply believing that something you take will exert some effect is often enough to manifest the realization of that effect.
Most people tend to underestimate the strength of placebo effects, but clinical researchers have methods to determine whether an effect being measured truly outpaces that of a placebo. The human psyche is so powerful that it’s difficult to overstate the importance of proper study design when assessing evidence.

The Next Ambien?
A literature search reveals there have been nine high-quality clinical research studies that probe the effects of CBN on human subjects. All these studies underwent the peer-review process, were published in respected scientific journals, and at bare minimum were placebo-controlled or performed in an appropriately blinded fashion.
It should be noted that most of these studies weren’t focused on sleep per se, and I suppose it’s possible that CBN could aid in some facet of sleep in a manner that eluded these experimental designs. Still, given all the anecdotal talk about CBN being “the next Ambien,” you’d think that there would at least be some drowsy effect noticed by any of the many participants that consumed massive doses of CBN. Yet almost all these people could not even discern any effect at all when taking THC-free preparations of CBN!
See the Appendix at the end of this article for a curated, chronological summary of what each of these nine studies entailed as well as their major conclusions. Of the nine high-quality clinical studies listed in the Appendix, only two might possibly indicate any signs of sleepy effects for CBN. So these merit further discussion and critical analysis.
Drugged, Drowsy, Drunk & Dizzy
Performed in the early 1970s, a study (listed as #4 in the Appendix) conducted at Escola Paulista de Medicina in Brazil involved five male volunteers in their late twenties who were orally given a different cannabinoid or combination of cannabinoids – they took placebo; 50mgCBN; or 25mgTHC + either 0mg, 12.5mg, 25mg, or 50mg CBN.
The publication describes four of the five volunteers as being “psychiatric residents at Escola Paulista de Medicina.” However, it is not clear to me whether this means these men were residents at the psychiatric hospital (as in, post-medical degree clinicians in-training). Or if they were residents at the psychiatric hospital (as in, patients living in a psych ward?!). I think there’s a decent chance that it’s the latter.
Recruiting psych ward inpatients for a study like this would probably be frowned upon by modern-day Ethics Review Boards, but this work was performed in Brazil nearly five decades ago when I suspect clinical research was performed a bit differently than it is today. If the study’s participants were also resident patients, then that should raise some concerns around how representative this cohort is to the general population – and whether the results could have been confounded by the participants concurrently taking other psychotropic medications.
Be that as it may, the participants were each asked to rate 66 subjective pairs – such as ‘happy-sad’, ‘drowsy-alert’, ’hot-cold’, & ‘drunk-sober’– and to indicate which they felt and how strongly they felt it on a scale from 1 to 4. Consuming 50mg of CBN alone was found to not be any different from taking placebo on any subjective effects or on heart rate. Significant differences, including “drowsy,” were only reported in four of the sixty-six subjective effects, and only when CBN was taken in combination with THC.[10] The four effects that reached statistical significance were “Drugged, Drowsy, Drunk, and Dizzy”.
In my opinion the significant differences that were found appear uninspiring to say the least. The interested reader can check out the results in Figure 1 of the published study here. The specific THC+CBN doses that reached significance appear haphazard, without much semblance of an expected dose-response. Sometimes the lowest and highest dose of CBN showed an effect but not the middle dose, or the lowest dose had an effect but not any of the higher doses. These observations are rather odd from a pharmacology perspective.
My biggest gripe with this study is that with their test scoring 66 items on four different CBN groups (equaling a grand total of 264 comparisons being drawn), some of them are bound to turn out statistically significant simply by sheer chance. That’s what we call a ‘Type I Error’ in statistics, and I suspect there may be some of that at play here. Basically, the larger the number of things you independently test against each other, the larger the likelihood of having some false positives in your dataset. Moreover, the extremely small sample size (there were only five people in this entire study!) increases the chance that these findings on CBN on ‘drugged, drowsy, drunk, & dizzy’ may be nothing more than statistical noise.
Recent Advances for Cannabinoid-Based Medicines & Insomnia
Next we turn to a recent Phase 1a/2b clinical trial (listed as study #9 in the Appendix) by the pharmaceutical start-up Zelira Therapeutics, although the experimental design, conduct, and analysis were independently performed by University of Western Australia’s Center for Sleep Science. Zelira’s drug, called ZTL-101, is a cannabis extract with three purified cannabinoids (THC+CBN+CBD) in sunflower oil intended for sublingual application. It is formulated as a THC:CBN:CBD ratio of 20:2:1.
The study enrolled 24 participants experiencing chronic insomnia, and for two weeks they took either a placebo or 0.5mL ZTL-101 (=10mgTHC+1mgCBN+0.5mgCBD) each night one hour prior to their desired bedtime. After the fourth night the participants were permitted to optionally double their dose to 1mL (=20mgTHC+2mgCBN+1mgCBD).
The study utilized a cross-over design, meaning that after two weeks all the patients receiving placebo were switched to ZTL-101, and vice versa. Each participant being part of both the placebo group and the drug group at different points helps control for inter-person variance and greatly improves the strength of a study like this.
The researchers assessed sleep quality in three distinct ways: Self-reported sleep diaries, actigraphy (wearing a watch which monitors nighttime movement) and a single night of polysomnography measurements (a comprehensive analysis of brain waves, heart rate, blood O2 levels, leg, and eye movement).
No statistically significant differences were uncovered between the placebo and ZTL-101 groups by the one night of polysomnography measurements. However, the sleep diaries and actigraphy measurements indicated that ZTL-101 significantly improved insomnia severity scores, reduced time it took to fall asleep, lessened nighttime wakefulness, increased total sleep time, and the patients reported waking up feeling more rested.
Overall, the results seem convincing enough to conclude that ZTL-101 significantly reduced insomnia severity scores and increased sleep quality in these patients. This is great! It is another piece of evidence supporting efficacy of cannabinoid-based therapies in sleep medicine. However, it seems much more likely that it’s really the THC that’s behind these effects, rather than the relatively miniscule amounts of CBN or CBD.
In many other studies THC-only preparations have indeed demonstrated self-reported sleep benefits (albeit with some seeming contradictions in the research around this).6 As this study only tested CBN in combination with THC and CBD, there is really no way to know until further comparative studies are performed. If more than 1000mgCBN/day did not exhibit any sort of noticeable sleepy effects, then it’s dubious that the 1-2mgCBN used in this study did much in that regard.

THC Alters Sleep Architecture
The endocannabinoid system (ECS) is entwined with our sleep and dreaming in ways that we are still striving to fully understand. We know that heavy cannabis users generally dream less (or at least, do not remember their dreams very well). And then upon abstention from cannabis they often have difficulty falling asleep, and once they do fall asleep, they tend to experience very vivid dreams. We know that the ECS helps to regulate circadian sleep-wake cycles and these observations point towards cannabis being able to induce alterations in our sleep architecture.
High-quality sleep studies have not found CBD to alter sleep architecture, and I’m not aware of any reported dream rebound effects after abstaining from chronic CBD use.[7] The main factor behind the sleep-related effects of cannabis seems to be THC. The research around how THC affects our sleep is a bit convoluted, but it is generally believed to shorten sleep onset latency (aka time it takes to fall asleep), to increase slow wave sleep, and to shorten the REM stages of sleep [6].
Consuming CBN isolate may weakly stimulate your ECS and this conceivably could help some facets of sleep. However, mechanistically this should not be any different than taking a very low dose of THC. Also, historically almost nobody has even tried CBN isolate because there will virtually always be some contaminating THC in high-CBN cannabis. If tickling the CB1 receptor is indeed how CBN works, then there probably wouldn’t be much real synergy between THC and CBN because the THC would strongly out-compete CBN for CB1 receptor binding. In other words, adding some CBN to a THC product (like most CBN products currently on the market) should not make it have sleepier effects.
So, if CBN isn’t sleep-inducing, then where did this rumor originate? Historically aged cannabis has been associated with producing more sedating effects. When it became more widespread knowledge that CBN is the major degradation product of THC, people began attributing these effects to the relatively higher CBN content that’s found in old flower.
Terpenes & Terpenoids
While it’s likely true that older cannabis tends to provide more sedating effects, I doubt that it’s the CBN that’s causing this. Cannabis is a complex mixture of many thousands of chemical constituents, and THC is not the only compound that converts into something else over time. Phytochemicals in plants are constantly degrading or changing in various ways as time passes. Acidic cannabinoids decarboxylate into their neutral counterparts or oxidize into various minor cannabinoids. Terpenes can incorporate oxygen atoms from the air converting them into terpenoids (such as linalool) which may exhibit comparatively more sedating effects.
The terms ‘terpene’ and ‘terpenoid’ are often used synonymously, but technically terpenes are exclusively hydrocarbons (meaning they consist of only carbons and hydrogens), while terpenoids contain additional functional groups, usually an incorporated oxygen atom.
Additionally, aged cannabis might have a higher ratio of sesquiterpenes (aka ‘heavy terps’; such as beta-caryophyllene) because the other main variety of terpene that the cannabis plant makes, monoterpenes (‘light terps’; such as limonene), are relatively more volatile and therefore evaporate away from plant matter more readily. The altered terpene profiles in aged cannabis could feasibly lead to more sedating or sleepy effects.
In-human research on terpene pharmacology is woefully lacking, but many terpenes have been demonstrated in animal models to produce significant analgesic and sedative effects.[8,9] Interestingly, many of these effects can be blocked by giving the rodent naloxone (aka Narcan), suggesting that some terpenes are at least partially working through our endogenous opioid system.
Note that terpenes themselves are not opioids as they are generally not able to activate opioid receptors. But some terpenes may increase our body’s production of natural opioids and/or act as positive allosteric modulators to opioid receptors. A positive allosteric modulator interacts with receptors in such a way that makes them more susceptible to activation by other compounds (which scientists refer to as “agonists”).

CBN Conclusions
CBN has seen a big surge in the cannabis market recently and manufacturers have jumped at the opportunity to widely advertise its anecdotal reputation for being a sleep-aid. However, based on the prior research that has been performed it appears that there are no special sleepy properties for this minor cannabinoid. Although there’s a lot of hearsay anecdotal support for CBN as a soporific, I remain dubious about these widespread claims.
The clinical research on CBN is still way too lacking to form a complete understanding of its pharmacology. While it’s possible that there are still yet-uncovered mechanisms of action for CBN that might aid sleep, I have not seen anything solid to support this theory. In all likelihood, the alleged sleep-assisting property of CBN is nothing more than an unfounded rumor that can be mostly attributed to two things. First is that historically people have noticed that older cannabis provided more sedating effects and mistakenly linked it to degraded THC. Second is that placebo can be one hell of a powerful drug!
Appendix: Nine Studies
What follows is a curated, chronological summary of nine high-quality clinical research studies that probe the effects of CBN on human subjects. All these studies underwent the peer-review process, were published in respected scientific journals, and at bare minimum were placebo-controlled or performed in an appropriately blinded fashion. I have briefly summarized what each of these studies entailed as well as their major conclusions:
CBN Study #1
- Location: North Carolina, USA; University of North Carolina School of Medicine Chapel Hill
- Principal Author: Dr. Mario Perez-Reyes
- Year: 1973
- Participants: Six healthy male volunteers
- The Study: Participants were given an i.v. and drug-free saline was infused directly into their bloodstream. The subjects were informed that at some unspecified time the saline would be replaced with a solution of CBN given at a constant rate of 1.2mgCBN/min. It took around 14mg of CBN injected directly into the blood for the participants to begin perceiving any subjective effects. They reported that the effects were enjoyable, but notably less intense than those elicited by THC. An increase in heart rate was observed at higher doses which serves as a confirmation that CBN is able to activate our CB1 receptors (CB1 activation is well known to do this…consuming THC increases your heart rate too!).[10]
CBN Study #2
- Location: Palo Alto, California, USA; Veterans Administration Medical Center
- Principal Author: Dr. Leo Hollister
- Year: 1973
- Participants: Six middle-aged male volunteers. All had some prior experience using cannabis.
- The Study: The volunteers were given 20-400mg CBN orally (in a chocolate cookie). No mental or physical effects of CBN were observed at any dose. This seemingly contrasts the findings of the previous CBN Study #1, where CBN was described as providing a light high and slightly increased heart rate when directly injected into the bloodstream. Taking 400mg of CBN orally should reach blood concentrations even higher than what was used in CBN Study #1, so the disparity in these results is a bit surprising.[11]
CBN Study #3
- Location: Palo Alto, California, USA; Veterans Administration Medical Center & Stanford University School of Medicine
- Principal Authors: Dr. Leo Hollister & Hampton Gillespie
- Year: 1975
- Participants: Fifteen healthy male volunteers. All had some limited prior exposure to cannabis use.
- The Study: The same researcher that performed CBN Study #2 came back to do another CBN study a couple years later. This time he gave the participants a cookie with 20mg THC plus either 40mg CBN or placebo. The 40mg CBN did not appear to do anything as there were no detectable differences between the ‘THC+CBN’ group vs. the ‘THC+placebo’ treatment groups. In the author’s words “…no quantitative or temporal difference was observed between THC-placebo and THC–CBN in terms of clinical effects. Qualitatively, each treatment produced identical effects.”[12]
CBN Study #4
- Location: Sau Paulo, Brazil; Escola Paulista de Medicina
- Principal Author: Dr. Isac Karniol
- Year: 1975
- Participants: Five male volunteers in their late twenties. Four of the five volunteers were psychiatric residents at Escola Paulista de Medicina. The other was an architect.
- The Study: Participants were orally given placebo, 50mgCBN, 25mgTHC, or THC in combination with various doses of CBN between 0-50mg. The participants were each asked to answer 66 subjective pairs (e.g. alert-drowsy, happy-sad, euphoric-depressed, etc.) with which they felt and to rate how strongly they felt it on a scale from 1-4. Figure #1 from the published study shows the results of a select four of the 66 subjective pair answers. Consuming 50mg of CBN was found to not be any different from taking placebo on subjective effects or heart rate. When the subjects received combinations of THC + CBN there were sometimes significant differences found, including “drowsy” with some THC+CBN combos.[13]
CBN Study #5
- Location: Australia; University of New South Wales
- Principal Author: Dr. Kevin Bird
- Year: 1980
- Participants: 161 healthy volunteers (122 men + 39 women). Most of the participants were college students. Ages ranged from 18-36 years old.
- The Study: The subjects were orally given 320µg/kg CBN (~25mg for an average-sized adult), either alone or in combination with 215µg/kg THC (= ~16mg), and then subjected to a series of cognitive, perception, reaction time, and motor function tests. The authors concluded that CBN was without effect on any of the parameters that they tested. Consuming CBN along with THC did not show any differences compared to taking THC alone.[14]
CBN Study #6
- Location: Palo Alto, California, USA; Veterans Administration Medical Center
- Principal Authors: Drs. Leo Hollister & Stig Agurell
- Year: 1981
- Participants: Twelve male volunteers between ages 18-40. All had prior experience using cannabis.
- The Study: Yet another one from Dr. Hollister’s team. This time they conducted a study focusing on whether CBN alters how our bodies metabolize THC. They used the same treatment condition as in their previous study (20mgTHC + either placebo or 40mgCBN, orally consumed). They did not observe any significant differences between the CBN vs. placebo groups.[15]
CBN Study #7
- Location: Los Angeles, California, USA; University of California Department of Medicine
- Principal Author: Dr. Henry Gong Jr.
- Year: 1984
- Participants: 59 healthy men between ages 21-32. All subjects were habitual cannabis users.
- The Study: Participants orally consumed 100mg, 600mg, or 1200mg CBN daily for 20 consecutive days. Subjective self-rated ‘highness scores’ were no different than that of placebo at any dose of CBN. Even at the highest 1200mg dose CBN did not alter heart rate. Twelve of the participants were then enrolled in a second part of the study where they received 400mg CBN in combination with 5mg THC. CBN did not appear to have any effect on heart rate or subjective high induced by THC.[16]
CBN Study #8
- Location: Uppsala, Sweden; Uppsalla University
- Year: 1987
- Principal Authors: Drs. Leo Hollister & Eva Johansson
- Participants: Six healthy male volunteers between ages 19-31. All were experienced cannabis users but abstained from cannabis use for at least 72 hours prior to the experiment.
- The Study: The focus of this study was to measure blood CBN levels following smoked vs. intravenous routes of administration (this sort of experiment is called a ‘pharmacokinetics’ or ‘PK’ study). Participants were given a 20mg i.v. infusion of CBN. Then, one week later, same participants smoked a THC-free joint containing 20mg CBN. While subjective effects were not really a focus of this study, the authors noted that neither smoked nor injected CBN produced any noticeable psychoactive effects.[17]
CBN Study #9
- Location: Australia; West Australian Sleep Disorders Research Institute & the University of Western Australia
- Year: 2021
- Principal Author: Dr. Jennifer Walsh
- Participants: 24 volunteers (20 women + 4 men) with chronic insomnia. Ages ranged from 25-70 years old.
- The Study: This recent clinical trial looked at ZTL-101 (a proprietary combination of THC+CBD+CBN at a ratio of 20:2:1) for the treatment of chronic insomnia. The participants took ZTL-101 sublingually daily for two weeks and it significantly improved insomnia symptoms and self-reported sleep quality compared to the placebo group.[18]
Copyright, Project CBD. May not be reprinted without permission.
Sorry, the comment form is closed at this time.